Research Project Methodogy Assignment
Methodology
This chapter will examine the methodological approach to the research project, discuss the research sample and data collection and subsequently outline ethical considerations as well as limitations to this research.
3.1 Research Philosophy and Approach
Whether consciously or unconsciously, every researcher is bound to make assumptions throughout the research process, which shape the form and outcome of their project (Burrell & Morgan, 1979; Crotty, 1998). Thus, it is vital to outline the philosophical underpinning of this research. Given the sensitive nature of the topic and complexity of mental health, this project understood that every participant had a unique view based upon personal perceptions, experiences and social conditioning. In addition, existent wellbeing programms were evaluated under consideration of employees individual experiences and perceptions. Thus, this dissertation followed both, a critical realist and an interpretivist philosophical approach (Saunders, Lewis & Thornhill, 2016). As an ontological framework, critical realism acknowledges the complexity and plurality of any human beings experiences, while not considering them epistemologically superior to underlying social realities. Because critical realism is open to both, qualitative and quantitative methods of enquiry, it furthermore lends itself well to a mixed methods design (Sayer, 2000).
Since a number of research questions have been developed on the base of existent research and literature, it would be possible to classify the theory development as deductive (Saunders et al. 2016). Yet, as this project also sought to find out, what research participants views are and to understand the nature of the problem (Saunders et al., 2016; p. 147) under the assumption that new insights may arise; this project also followed an inductive approach. Hence, as it combined inductive and deductive elements and moved back and forth between the two, the research followed an abductive approach (Saunders et al., 2016; Suddaby, 2006).
3.2 Research Design
For the purpose of this project, a concurrent mixed methods approach has been chosen as this allows for the separate use of qualitative and quantitative methods within one phase of data collection and provides a richer and more comprehensive response to the research question (Saunders et al., 2016, p.171). The use of two different techniques moreover allowed for a more comprehensive exploration of employers and employees perspectives (Bryman & Bell, 2015). The study combined elements of exploratory research as it set out to understand the relationship between stigmatizing attitudes, levels of support within organizational cultures, and disclosure of MHCs as well as evaluative research elements as this study looked at companys actions and their effectiveness (Saunders et al., 2016).
Both methods were considered equally important as each of them represents one partys views and thoughts around the topic. The data collected through each of these techniques was triangulated so that the results of each method could be compared and contrasted (Doyle, Brady and Byrne, 2009) and validity of the research increased (Saunders et al., 2016).
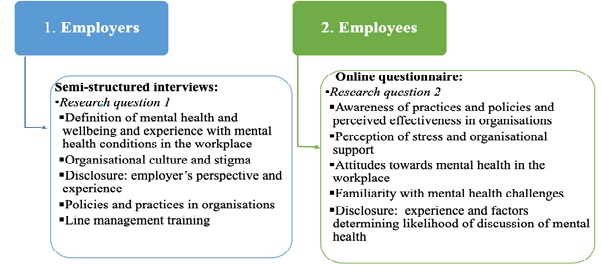
Figure 1. Research design mixed methods overview (own illustration)
3.2.1 Qualitative Data Semi-Structured Interviews
Semi-structured interviews were conducted with HR personnel and managers and business partners acting as senior and top management to gain an insight into employers views on the topic as well as their opinion on actions addressed to destigmatiation of mental health. This method was chosen because semi-structured interviews can be varied and adjusted to the context of the organization and the interviewee and hence allowed for an in-depth exploration (Saunders et al., 2016) of the policies and effects as well as a possible probing for perceptions around stigma and evaluations of organizational culture in this context.
The initial question catalogue (see Appendix B) was drafted based on R1 in relation to the literature discussed in chapter 2. Each interview broadly covered three themes, namely the organizational culture in relation to MH; prevalence of MHCs in the workplace and lastly the organizations P&Ps and interviewees perceptions thereof. Each interview began with an open question about what MH and wellbeing means to the interviewee in their role within the organization.
3.2.1.1 Research Sample Employers
Participants for the semi-structured interviews were chosen from a pool of individuals, who expressed their willingness to participate in the research by filling out an online form introducing this research project, which has been distributed through the corporate intranets. The participants were thus selected from a pool of volunteers, following a non-probability purposive sampling (Bryman & Bell, 2015). As the interviews aimed at portraying the employers perspective, the individuals chosen were either HR professionals or individuals in a (senior) management position as they were considered to have most inside in the organizations business management and organizational attitudes towards MH and wellbeing. Three of the interviewees did not only speak for their current organization but were considered experts as they take an active participation in developing wellbeing programmes inside their organisations, hence they offered a deeper and comparative look at the management of MHCs in other organizations as well as their own. As Table 1 outlines, participants came from the private, public and third sector as well as different industries, which attributes to the datas validity and reliability (Collis & Hussey, 2013).
|
Role |
Sector/Industry |
|
P1. HR Business Partner (Wellbeing Lead) - Expert |
Public Sector/Financial Holding |
|
P2. HR Advisor |
Private Sector/Professional Service Firm 1 |
|
P3. Managing Director (Wellbeing Lead) - Expert |
Private Sector/Insurance |
|
P4. HR Manager |
Private Sector/Professional Service Firm 2 |
|
P5. Owner |
Self-Employed Business Management Consultant |
|
P6. Chief Operations Officer (COO) |
Private Sector/Professional Service Firm 1 |
|
P7. Wellbeing Programme Manager/Expecrt |
Private Sector/Banking |
|
P8. HR Manager |
Private Sector/Legal |
|
P9. HR Business Partner (Wellbeing Lead) - Expert |
Public Sector/Health |
|
P10. Managing Director |
Private Sector/Digital Agency |
Table 1. List of interview participants (P1-10)
3.2.2 Quantitative Data Online Questionnaire
In order to reach a large number of employees, a self-completed online questionnaire was constructed using Google Surveys. The 22-item-questionnaire (see Appendix D) was designed against the background of research question R2 as well as hypotheses 1-4. The questionnaire was divided into three main parts.
The first part focused on the actions within respondents organizations as well as their perceptions thereof. A list of practices was adapted and extended from Henderson et al. (2013) to allow respondents to identify all practices offered by their employers. The second part focuses on respondents job and work environment. One item (In general, how do you find your job?) asking respondents to characterize their job on a scale between 1= extremely stressful to 4 = not at all stressful was adapted from Calnan et al (2004). The other four items within this section asked for respondents perceived levels of support from both colleagues and supervisors using a 5-point likert-scale (strongly agree to strongly disagree), and have been created on the base of the support-items of Karasek and Theorells (1992) Job Content Questionnaire. The third part of the questionnaire focused on respondents relationship with MH, asking them first to identify what they associate with the term mental ill health in the workplace from a list of MHCs adapted and extended from Henderson et al (2013). Subsequently, four items were used to measure attitudes towards mental illness in the workplace. These cover recommendation for a job, working alongside someone affected, concealment of mental illness at work and a person with MH issues in a leadership position. These items have been tested during preliminary conversations with HR/Talent departments, in which exploratory factor analysis using Varimax rotation in SPSS resulted in one dimension, thus granting validity. Lastly, the third section utilizes the level-of-contact-report (LCR) developed by Holmes et al. (1999). The LCR lists 12 situations of varying familiarity with mental illness with each of these situations given a rank score, resulting in an ordinal list from 1 to 12 from the least level of contact (1=I have never observed a person that I was aware had a mental illness) to the highest level (12=I have a mental illness). For the LCR, mental illness was replaced with MHC as this terminology was considered more appropriate for this research and to determine respondents levels of experience with MH. The LCR ranking has been validated and interrater reliability of rank order correlations was 0.83 (Holmes et al., 1999).
The questionnaire included three open space questions asking respondents to give their opinions on i) the effectiveness of their organizations mental health and wellbeing practices, ii) whether or not they believe these practices distinguish between stress, mental health and general wellbeing and why, and iii) any additional thoughts on the topic. While the other items generated numerical data, the questions still focused on opinions and attitudes, hence the overall data collected with this questionnaire can be classified as qualitative numbers (Saunders et al., 2016).
After the questionnaire was first drafted, it was sent to ten HR/Talent partners and managers as a pilot test to ensure that each item was clear and easy to understand and data collection worked properly. Upon this pilot study, small changes were made to ensure a logic structure and clarity of the questions before its distribution.

Figure 2. Questionnaire Design Process (own illustration))
3.3 Data Collection and Analysis
3.3.1 Qualitative Data
Prior to the interviews, all participants were informed of the research topic and its objectives via corporate e-mails. Information about the confidentiality and anonymity of participation was included in the e-mail and repeated verbally before the interview. To incorporate non-verbal communication and to hence ensure a better understanding, interviews were conducted via video conference services; namely, Skype, Zoom, Google Meets and 5 interviewees agreed for the interview to be recorded.
After the interviews, the obtained verbal data was transformed into written data through transcription, then the data was structured and coded, following a thematic analysis (Braun & Clarke, 2006) as outlined in Figure 3. The initial generation of codes followed a deductive approach as codes were identified in connection to R1. After initial themes were identified and relationships were established, the data was reviewed, following an inductive approach to identify new themes that did not relate back directly to R1. Subsequently themes were defined and an analysis report produced (see Chapter 4. Findings).

Figure 3. Process data analysis semi-structured interviews (own illustration) adapted from Braun & Clarke (2006)
Qualitative data obtained through the open-ended questions in the online questionnaire was analysed following an inductive thematic analysis approach.
3.3.2 Quantitative Data
The online questionnaire was distributed through corporate intranet as well as sent out to the interviewees and other individuals, who had expressed interest in the project, in an e-mail accompanying inviting recipients to distribute the survey to colleagues and friends if they felt that was something they would be confident with. The questionnaire was open and available online over a period of four weeks.
Subsequent analysis of the quantitative data obtained was done using SPSS. Two scales were identified one measuring the levels of support within an organizational culture and the other one measuring stigmatizing attitudes around MH in the workplace. Reliability was proven for both scales (for detail see Appendix A).
Descriptive statistics were produced using frequencies to analyze occurrences of MHCs in the workplace as well as to understand demographic distributions.
Moreover, correlations have been applied to understand the relationship between scales measuring stigmatizing attitudes and the level of familiarity participants note with MHCs as well as their perceived stress at work. Independent samples T-tests have been used to establish a relationship between participants likelihood to discuss MH in the workplace and i) the level of support they perceive and ii) their level of familiarity with MHCs. Independent T-tests and ANOVA have also been applied to the demographic data to obtain information about whether or not there are significant differences in relation to demographic groups and their likeliness to discuss MH in the workplace as well as stigmatizing attitudes.
3.4 Ethical Considerations and Limitations
This dissertation was designed in line with the Economic and Social Research Councils framework for research ethics core principles (ESRC, 2016). The topic of this research project is a highly sensitive one and it has been recognized that interviewees as well as participants of the online questionnaire were giving out personal information.
Hence, interviewees were informed about research objectives and ensured that information they shared will be treated anonymously and confidentially. The same applied to participants who filled out the online questionnaire. The questionnaire moreover included no mandatory items to ensure that all participants only answer questions they feel comfortable with which may be considered a limitation as it impacted the findings.
Despite its promise of an in-depth understanding of a subject matter, the complexity of a mixed methods approach may be understood as another limitation of this project as the time frame and context of this dissertation only allowed for a limited exploration and analysis of the data obtained. Further limitations will be discussed in the Discussions chapter.
