Clinical Governance and Patient Safety: Root Cause Analysis in Healthcare HSC3025
- Subject Code :
HSC3025
1. Problem Statement
The death of Roy Rodney Jacobs as highlighted within this particular coroner's report occurred from a series of communication failures and also lack of proper accountability among the people. The healthcare team was not at all accountable for their actions and they did not conduct effective communication which as a result led to the death of Roy Rodney Jacobs (Courts.qld.gov.au, 2017). The poor coordination as well as lack of clarity in roles has led to suboptimal care and also contributed to the patient's untimely death. Coordination and communication within a healthcare team is extremely important as without it a particular individual cannot find out the root cause that is leading to issues within the health of a patient (Gittell et al., 2020). The Root Causeway analysis aims to identify the contributing factors and also explore the root causes that can help prevent this scenario from occurring.
2. Context
From the overall case study, it can be found that effective communication in healthcare teams is critical and it helps in ensuring the patient's safety. Healthcare providers mostly rely on accurate as well as timely communication for planning and also delivering care particularly in complex cases (Ataguba & Ataguba, 2020). However, in this scenario, the Roy Jacobs case also showed a lot of complexities and it has been found that the healthcare team constantly failed to maintain clear and consistent communication. The case study highlighted that there were systematic issues in communication and accountability that contributed to the death of Roy Rodney Jacobs (Courts.qld.gov.au, 2017). This increased the likelihood of adverse events and also came out with negative outcomes.
3. Background Information
Roy Rodney Jacobs has been admitted to the hospital where he received the necessary care from various healthcare professionals. The case study has indicated that there were numerous instances of miscommunication and lapses in the transfer of care and unclear accountability among healthcare providers (Courts.qld.gov.au, 2017). These particular problems have culminated in inadequate patient monitoring and they failed to provide prompt clinical signs of deterioration and also lack of coordination. In the healthcare context, communication is extremely vital when multiple workers are involved and it helps in ensuring the safety of patients. Ineffective communication that has taken place in the case study led to fatal consequences.
4. Factors Contributing to the Event
The key factors that contributed to the adverse outcomes are:
Figure 1: The factors contributed to the failure of treatment
(Source: self-created)
- Constant failures in communication between the team members in the department thus resulting in gaps in the overall patient care plan and a lack of awareness about critical health information. As opined by Kwame & Petrucka (2020), communication aids in improving work progress in healthcare. Particularly, despite deteriorating conditions, none of the nursing staff in the hospital as well as medical experts has re-assessed his Q-ADDS scores. Henceforth, based on the case scenario, it can be addressed that as medical handover has not been conducted and confirmed, his care plan got compromised. The most significant reasons for Jacobs death were the inappropriate expertise in work handover and the improper role of work clarity. There was no effective communication between Dr. Maja and Dr. Nhapi as to the condition of the patient (Courts.qld.gov.au, 2017). Such communication breakdowns signify the presence of more fundamental cultural problems within the healthcare organisation.
- Lack of effective documentation led to gaps in the critical care information and impacted the overall healthcare treatment because of delayed decision-making. As per Dalglish et al., (2020), clear and concise documentation of patients' conditions helps in showcasing long-standing problems faced by patients. The case scenario demonstrates that lack of evaluation and documentation of Roys abnormal vital signs, his condition worsened leading towards significant challenges. As these issues have not been acted upon, like conducting ECG and cardiac assessment, the rate of danger in which Roy was in has been unable to be accessed.
- The roles and responsibilities of the overall team were unclear and this also led to inappropriate responses and showcased accountability issues. Lack of understanding of healthcare roles creates gaps in the quality of services (Endeshaw, 2021). The case scenario highlights that during the treatment of Roy at Cherbourg Hospital, there was no availability of permanent officers. Hence, as an effect, the existence of short-term locum doctors has impacted the clinical decisions impacting the traits of accountability management. This is especially true for those that run into healthcare systems that are rural or understaffed such as Cherbourg Hospital where temporary staff, or locums that may not have the familiarity of patient care protocols and also miss the hospital procedures (Courts.qld.gov.au, 2017).
- Lack of adequate supervision and training also leads to declination of junior staff progress in terms of providing care. According to Rawashdeh & Tamimi (2020), in association with training and development towards hospital staff members, support is obtained by patients during their clinical needs by reducing errors and issues. However, in the case of Roy, as nurses have not been provided with an adequate amount of training, they have failed to understand the severity of his condition leading towards major complexities. Most importantly, despite the presence of an early warning system within this organisation, as it has not been utilised to create awareness of situation deterioration, challenges have been faced. The death of Roy Rodney Jacobs also had much to do with technological failures. The Q-ADDS (Queensland Adult Deterioration Detection System) could have been that. The hospital was unable to properly monitor or react to changes in Jacob's health, each step of which relied on technological engagement. In Jacob's case, the early warning system was ignored, perhaps because healthcare workers relied on subjective information. It rendered them desensitised to technological warnings.
5. Fishbone diagram
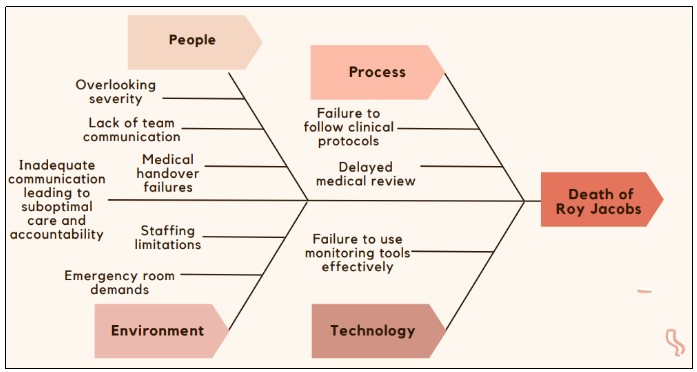
Figure 1: Fishbone diagram of showcasing the root causes of Jacobs death
(Source: Self-developed with idea from Courts.qld.gov.au, 2027)
Fishbone analysis has been considered as significant tool to find out the cause and effect of any situation. Through the above figure, the root cause analysis of Jacob's death has been evaluated.
6. Root causes
-
People
A lack of effective communication among nurses and doctors was necessary for such an issue. According to the case study, Dr Nhapi and Dr Maja failed to properly hand over the responsibility to each other. Trust in the clinical monitoring tools and ignoring the Q-ADDS scores were the major causes of Jacob's death due to the ignorance of people (Courts.qld.gov.au, 2027).
-
Process
The main process failure can be spotted from the failure of not following the Q-ADDS instructions in the treatment. According to the Fishbone Diagram, quality reduction from not following the documented process of treatment was another issue (Courts.qld.gov.au, 2027). These are the factors that have made the process failure unavoidable.
-
Environment
A lack of medical staff at the hospital was another reason for such issues. The process of treatment was purely based on temporary staff at the hospital and communication error was a problem in the overall situation. Lack of care from the emergency department has led to Jacobs death.
-
Technology
People working at the hospital did not follow the instructions of the Q-ADDS system. There was a lack of ECG and Cardiogram machines in the healthcare institution (Courts.qld.gov.au, 2027). These technological obligations have also influenced Jacobs death.
7. Propose a solution and implementation
Training of staff at the medical facility and the introduction of permanently trained staff is necessary to prevent such future issues (Willman et al., 2020). On the other hand, the introduction of new technologies and life support systems like ECG machines are necessary. This will certainly help in avoiding life loss due to the lack of a support system. The introduction of institutional protocol for proper documentation and following the instructions of the Q-ADDS system becomes necessary in the overall management (Courts.qld.gov.au, 2027). This process can certainly help in having an idea about the details of a patient.
The lack of experienced permanent personnel, and the general lack of sufficient staffing at Cherbourg Hospital, did much to contribute to Jacobs' death. Just as bad, the lack of senior oversight meant junior staff were left to stumble through complex medical situations without anyone to guide them (Willman et al., 2020). The safety of patients depends on having a well-supervised and adequately staffed healthcare environment particularly one in emergencies. Jacobs death is a reminder of the dangers that exist when understaffing and bad supervision combine.
The introduction of monitoring tools like Q-ADDS can help the medical professional learn about the overall condition of a patient. Doctors will be able to provide effective care and mineral support to the patient after identification of the issue that the patient is facing from such effective monitoring tools. According to Yi et al., (2022), the synthesis of each piece of information about the patient helps the doctors to learn about the exact show that the patient is facing at the hospital. Following these factors can help the medical professional to avoid Jacobs situation.
Efficient, clear and consistent documentation is one of the basic pillars of patient care, especially in complex cases involving several healthcare providers. Incomplete or inaccurate documentation compromises the care that the healthcare providers can offer (Ahmed et al., 2020). This case also emphasises the importance of meticulously recorded documentation in a healthcare facility to facilitate the updating of all patient information in real-time and to be able to be accessed by all staff involved in the patient's care.
The case scenario demonstrates that owing to a lack of implementation regarding risk assessment by healthcare staff, the death of Roy has occurred. Hence, the implementation of properly managed risk assessment tools and checklists might have led towards issue avoidance. The findings of Lyon et al., (2020) address that with assistance from risk assessment tools and checklists evidence-based treatment gets conducted providing patients with prominent healthcare assistance. Hence, based on Roys scenario, it can be addressed that strategic development for checklist and criteria selection can be applied to reducing damage and preventing deaths. In addition to this, a structured approach through properly guided consultation and preliminary actions can also help in managing these traits successfully.
The importance of continuous professional development and effective training for the health care workers, in particular, those working in critical caregiving environments cannot be ignored. In Roy Rodney Jacobs case, it was likely in part a lack of training and supervision of the nursing staff that caused them to fail to recognise, in light of the gravity of the patients condition, that he was succumbing to the effects of inhalational anaesthetic agents. However, the nurses and other healthcare workers must be constantly retrained to know when to catch early signs of warning and recognize how the hospital systems work, so such things never happen again in the future (Lyon et al., 2020). Ongoing education is a must for both technical skills and soft skills such as communication and teamwork, and healthcare organisations need to make available ongoing development programs that encourage this learning. Simulations in emergencies can enhance a team that responds, including Jacobs, and interprofessional education programs can contribute to creating a more collaborative and responsive healthcare team.
Apart from these approaches, in association with Tertiary Consultation and detection of Escalation Pathway evaluation, Roy would have been able to obtain health rather than facing death. Ahmed et al., (2020) have addressed that in association with the tertiary referral system, patients engage with highly skilled individuals specialised in handling critical medical conditions. Hence, it can be addressed that in association with Toowoomba Base Hospital, Roys treatment might have been commenced and conducted. Furthermore, the findings also highlight strategies like teaching staff knowledge about situations in which higher levels of risk are witnessed. It can be addressed that in association with these strategic initiatives, issues about complexity management might be restricted. The demonstration highlights that in association with strategic operations, management issues can be handled in a promising manner.
8. Reflective Evaluation
Response to Corners Report by Being Manager of the Hospital
Being the CEO of this hospital and after obtaining the report of Roy Rodney Jacobs death, I would have been deeply affected due to the system failure within my organisation and under my supervision. Hence, by undertaking immediate action, I would have been working to manage similar issues in the distant future without failure. The very first step that I might have taken will be evaluating the capability of existing staff members and present equipment. In an engagement with a proper enquiry team, I would have addressed the root cause of the failure and acted upon it. In addition to this, I would also have evaluated and managed the Q-ADDS system and escalated the concerns regarding the issues of the vital sign detection process.
Apart from these initiatives, I would also look after the referral programmes and locum protocols for handing over critical patients in terms of the presence of ineffective service within the institute. This initiative might provide my organisation with assistance in evaluating our promising approach and concern towards patients and their severity. This sole accident within my organisation might help me in setting specific rules and regulations utilising regular auditing facilities for institutional system management. Keeping the vital response team on standby in case of handling critical cases and conducting definitive actions can also help me as well as my organisation in improving the organisational approach successfully. Therefore, all I can say is, with assistance from these major initiatives and actions I might have improved organisational operating setups in a more promising manner by making them more patient-centric.
Observation about Patient Error
In consideration of this context, I can remember a different context in which I was involved. As an on-floor doctor, I have prescribed a patient a certain amount of medication based on their health condition. However, due to the miscommunication between the nursing and pharmacy departments, dosage errors have been witnessed impacting patients' health drastically. However, as I have been present in the scenario, witnessing unusual side effects on patients, the situation has been handled quickly before it escalated. Owing to my efficiency in diagnostics and the evaluation of the parameters, that severity has been omitted which was a complete failure in the case of Roy Rodney Jacob.
In terms of handling the critical condition, initially, I contracted my next senior and asked for re-evaluating my evaluation based on the patient's clinical report after medication. After that, I in association with the enquiry committee engaged with the nursing team and pharmacy department to seek the root cause of this incident. Most importantly, with prominent training towards the nursing team and providing them with strict instruction, I have been able to reduce the chance of a similar situation from then onwards with immediate effectiveness. As I have obtained proper training in patient management processes and evaluating their needs, with professionalism I have effectively managed the challenge more constructively.
Summary
It can be surmised that the death of Jacob is a communication and information-sharing failure from the side of the healthcare unit. Taking the help of effective technology for learning about the situation of the patient would have helped in saving the life of the patient in this case. Introduction of such an effective. Introduction of an effective training process for the introduction of permanent staff and development of technology-based treatment system can help in such issue reduction.
Are you struggling to keep up with the demands of your academic journey? Don't worry, we've got your back!
Exam Question Bank is your trusted partner in achieving academic excellence for all kind of technical and non-technical subjects. Our comprehensive range of academic services is designed to cater to students at every level. Whether you're a high school student, a college undergraduate, or pursuing advanced studies, we have the expertise and resources to support you.
To connect with expert and ask your query click here Exam Question Bank
