Complex Clinical Care 3803NRS
- Subject Code :
3803NRS
3803NRS Complex Clinical Care
A2 Written Assignment Nursing Care Plan 2000 words
Weighting: 50%
Due Date: see course profile
Aim: In this assessment item you will have the opportunity to apply your critical thinking skills to develop a nursing care that focuses on clinical deterioration and the potential for failure to rescue. Nursing care planning enables nurses and student nurses to demonstrate their clinical decision- making capabilities and supports safe evidence-based practice.
This assessment item will assess:
Learning Outcome 1: Demonstrate theoretical knowledge, practical skills, and interprofessional and cultural capabilities that underpin safe and competent nursing care for people with high acuity and/or complex needs
Learning Outcome 2: Create an evidence-based plan of nursing care for the person with high acuity and/or complex needs
Learning Outcome 3: Demonstrate safe, reflective, evidence-based, and person-centered nursing care for people with high acuity and/or complex needs, which is consistent with the Nursing and Midwifery Board of Australia (NMBA) Registered Nurse Standards for Practice
Task Description
Within the online content, you have explored complex nursing care, with a focus on acute deterioration and the importance of nursing care plans. For this task, you need to examine a case study and create an appropriate nursing care plan for the patient in the case study (2000 words).
Instructions:
Select ONE of the following case studies, and with reference to appropriate scholarly literature:
- Identify TWO (2) actual or potential priority problems related to failure to rescue described in the selected case study. For each problem, justify your choice as a priority (e.g., by referring to the patients assessment data in the selected case study and to appropriate literature)
- For EACH priority problem, identify ONE (1 ) SMARTgoal for care of the selected patient (total 2 goals). Remember a SMART goal is specific, measurable, attainable, realistic, and timely
- For EACH goal, describe TWO (2) evidence-based nursing interventions you would implement to meetthe goal (total 4 interventions). For each nursing intervention, justify your choice by referring to appropriate literature.
- For EACH goal, identify the expected outcomes and describe your evaluation approach (e.g., how, and when, would you evaluate whether your interventions have been effective or not?)
- Analysethe impact of failure to rescue on the patient, their family, and the health care
Choose EITHER Case Study 1 OR Case Study 2
Case Study No. 1 - Rapid Deterioration of Peter Mills at Griffith University Hospital Patient Profile
Name: Peter Mills Age: 71
Gender: Male
Medical History : Hypertension, Type 2 Diabetes, Chronic Kidney Disease (Stage 3), Angina, Atrial Fibrillation (AF), Chronic Heart Failure (CHF) and Chronic Obstructive Pulmonary Disease (COPD). His heart failure has been stable.
Social History : Peter lives with his wife Carol in a low story house in Kedron. Both their children live interstate and visit several times a year. Peters wife has dementia, and Peter is her main carer. They have weekly visits by the community nurse and Carol attends weekly respite care. Peter is a retired Accountant and relies on his superannuation for income.
Peter currently smokes 5-10 cigarettes a day and has a 40-year history. Peter has a moderate alcohol consumption with up to 2 standard drinks per day. Peter walks to the shops daily with Carol and is independent with all his cares. He reports occasional shortness of breath on exertion.
Medications
Peter takes Tiotropium (maintenance medication) for COPD, whilst using salbutamol as a reliever. Peter states he often forgets to use the Tiotropium. Peter also takes Captopril 12.5mg three times a day and was commenced on Metformin 500mg twice a day on his last admission but takes the medication irregularly and only when his blood sugar is high. He normally takes 20 mg Lasix (Frusemide) mane, Digoxin 0.125 mg nocte, however he has missed his medications for the past 3 days
Presenting Condition
Peter Mills was admitted to Griffith University Hospital on January 16, 2025, at 1630 with a report of a worsening infected ulcer on his right great toe and increased shortness of breath. Peter cannot recall injuring his right great toe. He attended his general practitioner two weeks ago and the practice nurse dressed his toe. He was required for second daily dressings but unfortunately, was unable to attend due to caring for Carol. He has been washing the toe daily and dressing it with plasters.
He reported a two-week history of lethargy, cough, increased shortness of breath, dizziness and increased peripheral oedema, notably in bilateral lower legs. Both lower legs are noticeably discoloured and mottled.
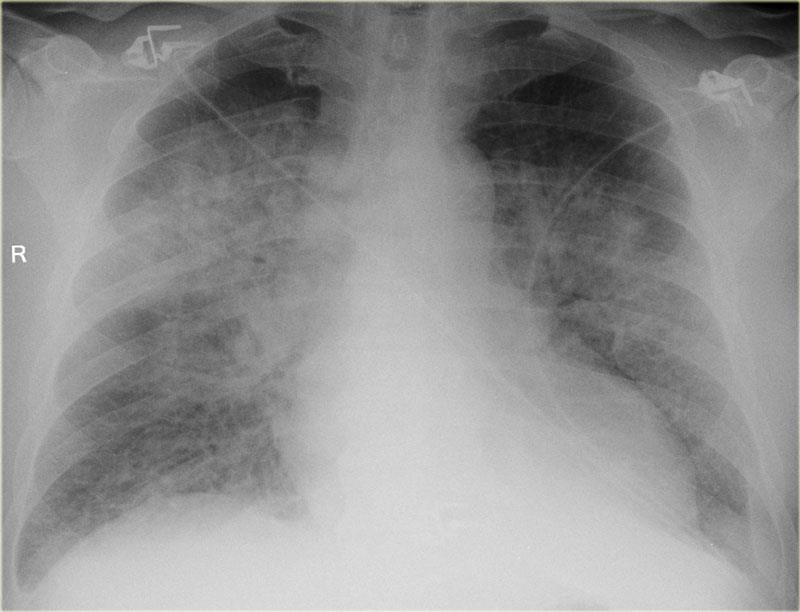
Peter has multiple co-morbidities and is currently under the care of a respiratory physician but has not consulted his endocrinologist for over a year. Peter was hospitalised once in the last year for increased shortness of breath related to COVID. His respiratory medications were modified at his last admission. Chest X-ray on admission shows consolidation and his BGL 16.2 mmol/L.
ISOBAR Communication Approach
In Peter Millss case, the ISOBAR approach was used to facilitate communication between the registered nurse (RN), Lucy, and the registered medical officer (RMO) covering the late shift. Lucy introduced herself to Peter at the commencement of the shift, gathered key patient information, and
ensured the patients identity. Lucy confirmed Peters current health issues, medications, and relevant medical, surgical and psychosocial history
I Introduction:
RN Lucy contacted the RMO at 20:30hrs, introduced herself, and identified the ward she was calling from and the relevant patient.
S Situation:
Peter was noted to have a QADDS score of 6 at 20:15hrs (Case Study 1 Adjunct Data QADDS). RN Lucy outlined Peter Millss history and presenting complaint, highlighting worsening shortness of breath, reported dull chest ache, low oxygen saturation, hypotension, tachypnoea, presence of atrial fibrillation, increasing BGL. Peter has passed urine once today.
Lucy has also noted, increased pain in Peters right great toe with noted redness, purulent exudate and pain on palpation. Lucy has noted bilateral mottling, discoloration and oedema of the lower legs.
O - Observation:
RN Lucy provided observations, including, BGL= 16.2, right great toe wound, increasing lethargy, bilateral crackles on lung auscultation and the titration of supplemental oxygen to maintain SpO2 between 88- 92%, via nasal prongs at 0.5-2L/min1.
- BP 145/100 mmHg (post nocte Captopril)
- HR 122bpm and irregularly irregular
- Respiratoryrate 28 bpm
- Temperature 378
- SpO286%
- CapillaryRefill greater than 3 seconds
- GlasgowComa Score 13/15
B - Background:
RN Lucy shared Peter Mills's relevant medical background, including his co-morbidities, recent hospitalisations, medications and social history
A - Assessment:
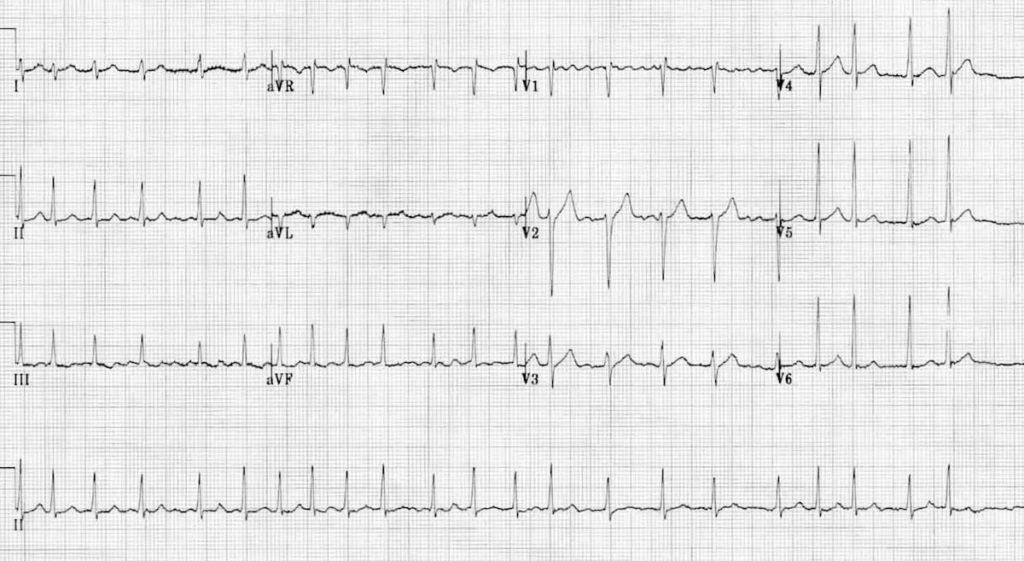
RN Lucy discussed her assessment findings, including the need for diuretic therapy to manage fluid overload and the presence of new-onset atrial fibrillation on the ECG.
Chest X-ray (Case Study 1 Adjunct Data)
Full Blood Test Results (Case Study 1 Adjunct Data) ECG (Case Study 1 Adjunct Data) Urinalysis (Case Study 1 Adjunct Data)
R - Recommendation:
RN Lucy immediately notified the team leader and planned a medical resident review within 30 minutes. Peter was commenced on hourly observations.
RMO reviewed Peter at 21:45 and ordered a stat IV dose of Frusemide 40mg and to monitor vital signs hourly.
Deterioration:
Despite RN Lucys utilisation of the ISOBAR communication approach, Peter Mills's condition continued to deteriorate rapidly over the next 2 hours. His oxygen saturation revealed minimal improvement, and he required increased oxygen support. He remained tachypnoeic, hypertensive and tachycardic. He became increasingly dyspnoeic and fatigued, cooling peripherally with a prolonged capillary refill time and reduction in GCS, arterial blood gas indicates respiratory acidosis.
Vital signs
- HR126bpm irregularly irregular
- BP157/105 mmHg
- Respiratoryrate 26 bpm
- Temp-5
- SpO285% on 2L/min Oxygen
- Capillaryrefill time > 3 seconds
- Conscious-responding to voice
- ArterialBlood Gas pH: 32 (7.35 - 7.45)
- PaO2:58mmHg (80 - 100 mmHg)
- PaCO2:52mmHg (35 - 45 mmHg)
- HCO3-: 26 mEq/L (22 - 28 mEq/L)
Please refer to the document Case Study 1 Adjunct Data for further information relating to this scenario and its relevant data.
Case Study 1: Peter Mills Adjunct Data
QADDS Score
- BP =0
- HR= 2
- RR =1
- Temperature= 0
- Oxygensaturations= 2
- Consciousness= 1
Total score = 6
Full Blood Count
- Haemoglobin(Hb)
- Result:120 g/L
- ReferenceRange: 130 - 170 g/L
- Haematocrit(Hct)
- Result:38%
- ReferenceRange: 38 - 50%
- RedBlood Cell Count (RBC)
- Result: 4.2 x 10^12/L
- ReferenceRange: 5 - 6.5 x 10^12/L
- WhiteBlood Cell Count (WBC)
- Result: 8.5 x 10^9/L
- ReferenceRange: 4 - 11 x 10^9/L
- PlateletCount (Plt)
- Result: 250 x 10^9/L
- ReferenceRange: 150 - 450 x 10^9/L
- MeanCorpuscular Volume (MCV)
- Result:90 fL
- ReferenceRange: 80 - 100 fL
- MeanCorpuscular Haemoglobin (MCH)
- Result:28 pg
- ReferenceRange: 27 - 34 pg
- MeanCorpuscular Haemoglobin Concentration (MCHC)
- Result:32 g/dL
- ReferenceRange: 32 - 36 g/dL
- RedCell Distribution Width (RDW)
- Result:12%
- ReferenceRange: 5 - 14.5%
Chest X Ray Anterior/Posterior View Upright.
12 Lead ECG
Urinalysis Results for Peter Mills (Prior to Diuretic Therapy)
- Colour:Dark Orange
- Clarity:Cloudy
- Odour:Slight odour of Ammonia
- Volume:400mL in last 24hrs fluid restriction?
- SpecificGravity: 035
- pH:6 to 7
- Protein:++ proteinuria
- Glucoseand Ketones: within the normal range
- Bilirubinand Urobilinogen: within the normal range
- Nitritesand Leukocytes: within the normal range
Case Study No. 2 Aisha Khan Hospital Admission for Stable Hypoglycaemia at Griffith
University Hospital
Patient Profile
Name: Aisha Khan Age:55 Gender: Female
Medical History : Type 2 Diabetes Mellitus, hypertension, and hyperlipidaemia. Aisha weighs 92.5kg, her height is 167 cm, and her waist circumference is 106 cm. Aisha takes Optisulin (insulin) 30 units at night and Metformin extended release for blood glucose control, Captopril for hypertension (target systolic < 120>
Social History: Aisha is married and lives with her spouse Emad in a suburban home, working full- time as a project manager in a local IT company. Aisha is mother to two adult children who have moved out of home. Aisha and her husband try to make healthy food choices. Aisha tries to incorporate regular physical activity into her routine but has recently dropped off her exercise due to increasing work demands. Work pressures have also meant she is not monitoring her blood glucose levels routinely.
Presenting Condition
Mrs Aisha Khan presented to Griffith University Hospital Emergency Department (ED) at 4 a.m. on November 1, 2024, with symptoms of hypoglycaemia stating she felt lethargic, following a recent viral illness, including 24 hours of vomiting and diarrhoea. Aisha still took her Optisulin the night before with a couple of biscuits. On admission Aisha had a blood glucose level of 3.1. Aisha was administered IV antiemetic medication and IV Glucagon. The ED RMO inserted a peripheral intravenous cannula and ordered IV sodium chloride 0.9% with glucose 5% 1 Liter, delivered at 125 ml/hr. At 9 a.m. (same day), Aisha was transferred to the medical ward for the continuance of IV fluid therapy and stabilisation of blood glucose.
ISOBAR Communication Approach
In Aisha Khan's case, the ISOBAR approach facilitated communication between the registered nurse (RN), Omar, and the registered medical officer (RMO) covering the morning shift. Omar introduced himself to Aisha on transfer to the ward, gathered key patient information, and confirmed the patient's identity in addition to Aishas current health issues, medications, and relevant history.
Introduction: During the morning medical round RN Omar, introduced himself, and Aisha Khan, a 55- year-old female, who was admitted with hypoglycaemia and dehydration due to a recent viral illness accompanied by vomiting and diarrhoea for 24hrs, before admission. No further vomiting or diarrhoea since presenting to the Emergency Department at 4 am.
Situation: Aisha has a known history of Type 2 Diabetes Mellitus coexisting with hypertension and hyperlipidaemia. Current blood glucose level currently is 4.8.
Observation: Upon admission to the medical ward, Aisha 's baseline assessment was:
Vital Signs:
Blood pressure 132/82 mm Hg (post oral dose of Captopril) HR 87 bpm
RR 17 bpm
SpO2 of 97% on room air Temperature, 36.6 degrees centigrade
Neurological Status: GCS 15, mildly lethargic
General Examination: pink and well perfused, capillary refill time < 2>
Other Lab Results: Normal serum creatinine and electrolyte levels. QADDS score: 0
Background : Aisha has a 2-year history of Type 2 Diabetes Mellitus, hypertension, and hyperlipidaemia. Up until recently, Aisha had consistently monitored blood glucose levels. Most recent documented HbA1c result was 7% (53mmol/mol).
Assessment : Aisha is currently stable, with Blood Glucose Level within normal range.
Recommendations: Further evaluation revealed that Aisha had been missing meals before the viral illness due to work pressure and an increased feeling of being overwhelmed and helplessness. Aisha revealed she had also forgotten to regularly test her blood glucose levels and take
Metformin. She is still taking her regular Optisulin at night after a snack before bed. Referral to a Diabetic Educator to discuss recent difficulties in monitoring blood glucose levels was commenced and a planned visit by the social worker.
Approximately 2 hours later, Aisha experienced a sudden deterioration. Aisha reported
feeling nauseated and dizzy before starting to slur speech. RN Omar notified the medical officer to report the observations and assessment data gathered using a primary survey:
Airway: patent
Breathing: borderline bradypnea (8 bpm), shallow breathing, SpO2 91-92% on room air
Circulation: Hypotensive - Blood pressure 94/50 mm Hg, bradycardic, 49 bpm
Disability: decreased level of consciousness, eyes = 2, Voice = 3, Motor = 5 GCS of 10/15, Blood Glucose Level = 1.676 mmol/L (venous sample)
Exposure: Temperature 36.5 degrees centigrade QADDS score: E
Please refer to the Case Study 2 Adjunct Data for further information relating to this scenario and its relevant data.
Case Study 2 Aisha Khan Adjunct Data
Breathing: borderline bradypnea (8 bpm), shallow breathing, SpO2 91-92% on room air
Circulation: Hypotensive - Blood pressure 94/50 mm Hg, bradycardic, 49 bpm
Disability: decreased level of consciousness, eyes = 2, Voice = 3, Motor = 5 GCS of 10/15, Blood Glucose Level = 1.676 mmol/L (venous sample)
Exposure: Temperature 36.5 degrees centigrade QADDS score: E
QADDS #1
BP = 0
HR = 0
RR = 0
Temperature = 0 Oxygen therapy = 0 Consciousness = 0 Total score = 0
QADDS score #2
Respiratory Rate = E
Consciousness = AVPU E unresponsive, GCS 10
Pulse Oximeter

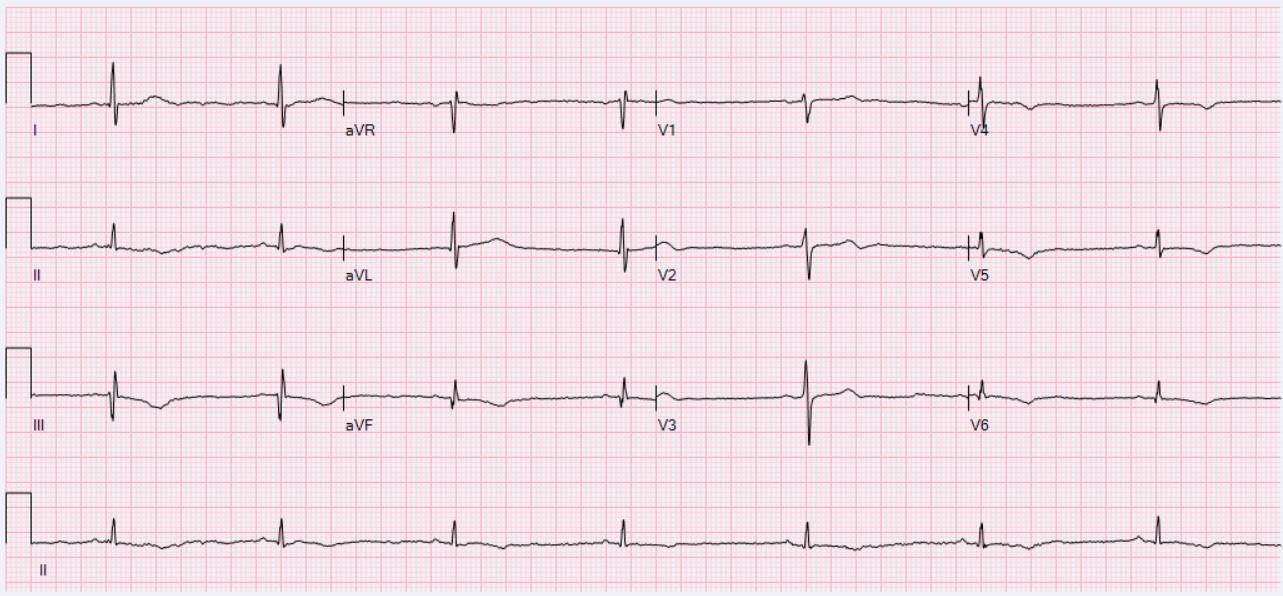
12 Lead ECG
Urea and Electrolyte Results
Sodium 132 mmol/L Potassium 3.8 mmol/L Chloride 99 mmol/L
Bicarbonate 23 mmol/L Urea 11.1 mmol/L
Creatinine: Female 109 ?mol/L eGFR 82 ml/min/1.73m?2;
3803NRS Complex Clinical Care
A2 Written Assignment: Nursing Care Plan MARKING RUBRIC
|
3803NRS A2 Assessable Elements |
EXEMPLARY Exceptionally high quality of performance or standard of learning achievement. |
ACCOMPLISHED High-quality performance or standard of learning achievement. |
DEVELOPING Satisfactory quality of performance or standard of learning achievement. |
BEGINNING Unsatisfactor y quality of performance or standard of learning achievement. |
TOTAL MARK |
|
Criterion One Identify two potential/actual priority problems related to failure to rescue and justify the selection |
Exceptionally high standard as evidenced by accurate identification of a priority problem and comprehensive and evidence- informed justification that includes reference to all failure to rescue cues that led to identifying that problem as a priority. |
High-quality standard as evidenced by mostly accurate identification of a priority problem and detailed and evidence-informed justification that includes reference to most of the failure to rescue cues that led to identifying that problem as a priority. |
Satisfactory standard as evidenced by an adequate identification of a priority problem and sound and evidence-informed justification that includes reference to some failure to rescue cues that led to identifying that problem as a priority, although some errors were evident |
Unsatisfactory standard as evidenced by the limited description of a priority problem and minimal or no failure to rescue cues and evidenced- informed justification, with many errors evident |
/12 |
|
Mark allocation PACC 1 |
6 |
5 |
3-4 |
0-2 |
|
|
Mark allocation PACC 2 |
6 |
5 |
3-4 |
0-2 |
|
|
Criterion Two Identify and prioritise two goals (G) for care using SMART structure |
Exceptionally high standard as evidenced by a clear and comprehensive identification and appropriate prioritisation of goals for the patients care |
High-quality standard as evidenced by clear identification and appropriate prioritisation of goals for the patients care |
Satisfactory standard as evidenced by an adequate identification and appropriate prioritisation of goals for the patients care |
Unsatisfactory standard as evidenced by limited identification and appropriate prioritisation of goals for the patients care |
|
|
Mark allocation G1 |
6 |
5 |
3-4 |
0-2 |
/6 |
|
Mark allocation G2 |
6 |
5 |
3-4 |
0-2 |
/6 |
|
Criterion Three Describe four relevant nursing interventions and provide an evidence-based rationale for |
Exceptionally high standard as evidenced by a clear and succinct description of the nursing intervention |
High-quality standard as evidenced by a fairly clear and succinct description of the nursing intervention appropriate for the specific health care |
Satisfactory standard as evidenced by an adequate description of four nursing interventions appropriate for the |
Unsatisfactory standard as evidenced by a limited description of nursing intervention that is not |
|
3803NRS A2 Assessable Elements |
EXEMPLARY Exceptionally high quality of performance or standard of learning achievement. |
ACCOMPLISHED High-quality performance or standard of learning achievement. |
DEVELOPING Satisfactory quality of performance or standard of learning achievement. |
BEGINNING Unsatisfactor y quality of performance or standard of learning achievement. |
TOTAL MARK |
|
Nursing intervention |
appropriate for the specific health care needs of the patient in the case study. Exceptionally high standard as evidenced by synthesis and accurate integration of high quality, credible evidence to provide a comprehensive and considered rationale for each nursing intervention; regular reference is made to the specific needs of the patient in the case study |
needs of the patient in the case study. High-quality standard as evidenced by some synthesis and integration of good quality, credible evidence to provide a logical rationale for each nursing intervention; regular reference is made to the specific needs of the patient in the case study |
specific health care needs of the patient in the case study. Satisfactory standard as evidenced by attempting synthesis and integration of reasonable quality, credible evidence to provide a sufficient rationale for each nursing interventions; o ccasional reference is made to the specific needs of the patient in the case study |
appropriate for the specific health care needs of the patient in the case study. Unsatisfactory standard as evidenced by a lack of synthesis and integration of evidence resulting in an undeveloped rationale for nursing interventions; little reference is made to the specific needs of the patient in the case study |
|
|
Mark allocation NI1 |
6 |
5 |
3-4 |
0-2 |
/6 |
|
Mark allocation NI2 |
6 |
5 |
3-4 |
0-2 |
/6 |
|
Mark allocation NI3 |
6 |
5 |
3-4 |
0-2 |
/6 |
|
Mark allocation NI4 |
6 |
5 |
3-4 |
0-2 |
/6 |
|
Criterion Four Discuss expected outcomes for interventions and provide description of how this outcome would be evaluated |
Exceptionally high standard as evidenced by a clear and comprehensive identification of expected outcomes and high-level discussion of how this outcome is evaluated with reference to the case study |
High quality standard as evidenced by clear and appropriate identification of expected outcomes and a good discussion of how this outcome is evaluated with reference to the case study |
Satisfactory standard as evidenced by an adequate identification of expected outcomes and adequate discussion of how this outcome is evaluated with reference to the case study |
Unsatisfactory standard as evidenced by limited identification of expected outcomes and inadequate discussion of how this outcome is evaluated with limited or no reference to the case study |
/12 |
|
Mark allocation |
11-12 |
8-10 |
6-7 |
0-5 |
|
|
Criterion Five |
Exceptionally high standard as evidenced by a |
High-quality standard as evidenced by a clear analysis of the |
Satisfactory standard as evidenced by an |
Unsatisfactory standard as evidenced by |
/12 |
|
3803NRS A2 Assessable Elements |
EXEMPLARY Exceptionally high quality of performance or standard of learning achievement. |
ACCOMPLISHED High-quality performance or standard of learning achievement. |
DEVELOPING Satisfactory quality of performance or standard of learning achievement. |
BEGINNING Unsatisfactor y quality of performance or standard of learning achievement. |
TOTAL MARK |
|
Analyse the impact of failure to rescue on the patient, their family, and the health care system. |
clear and comprehensive analysis of the impact of failure to rescue on the patient, their family, and the health care system |
impact of failure to rescue on the patient, their family, and the health care system |
adequate analysis of the impact of failure to rescue on the patient, their family, and the health care system |
limited analysis of the impact of failure to rescue on the patient, their family, and the health care system |
|
|
Criterion Six Presentation, grammar, and academic writing |
Exemplary demonstration of academic writing standards; Exemplary sentence and paragraph structure, with few, if any errors , exemplary and overall logical flow, that indicates a sophisticated ability to communicate ideas effectively |
High-quality demonstration of academic writing standards; appropriate sentence and paragraph structure, with some errors and overall logical flow, that indicates an effective ability to communicate ideas effectively |
Sufficient demonstration of academic writing standards; Developing sentence and paragraph structure, and/or some errors disrupt the logical flow or communication of ideas |
Does not comply with academic writing standards; Poor sentence and paragraph structure and poor logical flow demonstrates an i nability to communicate ideas effectively |
/12 |
|
Mark allocation |
11-12 |
8-10 |
6-7 |
0-5 |
|
|
Criterion Seven Evidence and referencing |
Exceptionally high standard as evidenced by exemplary use of APA 7 format in- text and reference list with no errors. 9 or more high- quality, appropriate references used |
High-quality standard as evidenced by the consistent use of APA 7 format in-text and reference list with minimal errors. 7-8 quality, appropriate references used |
Satisfactory standard as evidenced by the developing use of APA 7 format in-text and reference list, but with several errors. Less than 8 appropriate references used |
Unsatisfactory standard as evidenced by the beginning or absent use of APA 7 format in- text and reference list with many errors . Less than 5 references used or used several low-quality references |
/16 |
|
Mark allocation |
15-16 |
12-14 |
9-11 |
0-8 |
|
|
TOTAL |
/100 |
||||
